
Dental Insurance
Choose from an extensive network of dentists and save with economical group rates.
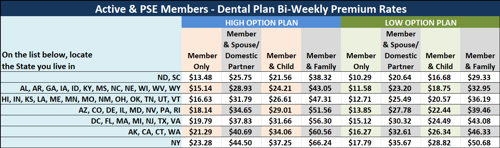
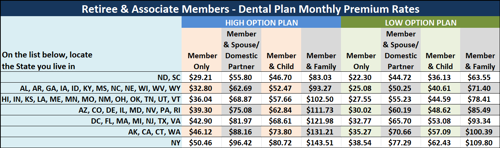
Taking care of your teeth is vital to your overall health. The good news is you can now take a bite out of your dental bills when you sign up for our Dental Insurance Plan. Simply choose the plan that best suits you and your family, see options in the benefits summary below.
For questions call 1 (800) 422-4492,
Monday through Friday, 8:30 AM to 5 PM (ET)
| Coverage Type | Low Option-Reimbursement Plan | High Option-Reimbursement Plan |
|
Type I: Preventive Services Cleanings, Oral Examinations, X-Rays, Sealants |
100% In- Network 100% Out-of-Network |
100% In- Network 100% Out-of-Network |
|
Type II: Basic Services Fillings, Oral Surgery, Extractions |
50% In- Network 50% Out-of-Network |
80% In- Network 80% Out-of-Network |
|
Type III: Major Services Bridges, Dentures, Crowns, Periodontics, Implants |
50% In- Network 50% Out-of-Network (12 month waiting period) |
50% In- Network 50% Out-of-Network (6 month waiting period) |
| Type IV Benefits: Orthodontia (Optional coverage for both adults and children) |
50% In- Network 50% Out-of-Network (12 month waiting period) |
50% In- Network 50% Out-of-Network (6 month waiting period) |
To add optional Orthodontic Coverage, check off "Yes" on the Enrollment Form.
Your selected premium will automatically be increased by 10%.
Dental Plan is not available in the following states: MT,NH,OR,SD, LA, AK.
| Calendar Year Deductible | No Deductible for - Type I Benefits, $100 per person, $300 per family - Type II and Type III benefits, combined |
| Calendar Year Maximum | $1,500 per person for all covered services |
| Lifetime Maximum | $1,000 for Orthodontic services, if Optional Orthodontic Coverage is selected |
Please Note:
You must notify The Voluntary Benefits Plan of any address change for you, your dependents and/or beneficiaries, and any change in employment and union membership status change, life status change (i.e., marriage, divorce, beneficiary or name change), or benefit changes requested. Notice must be in writing.
![]() Administered By:
Administered By:
Voluntary Benefits Plan
P.O. Box 12009
Cheshire, CT 06410
Phone: 1-800-422-4492
Fax: 1-203-754-7847
This plan is underwritten by Metropolitan Life Insurance Company, New York, New York. This summary is a brief description of benefits only and is subject to the terms, conditions, exclusions and limitations of Group Policy No. 122705.